Leishmania
(Leishmania infantum)
Leishmania infantum, transmitted by phlebotomine sand flies, causes a severe form of visceral leishmaniosiso in dogs in many parts of the world. If left untreated or treated at a progressive stage, leishmaniosis can be fatal. Dogs act as primary reservoirs L. infantum for human infection.
| Parasite: Leishmania infantum (Note: several other species of Leishmania may infect dogs worldwide [1]) |
| Common name: Leishmania |
| Host: Dogs, cats, humans |
| Incubation period: Weeks to years |
| Location in host: Reticuloendothelial system (phagocytic cells) |
| Distribution: South America, Middle East, Southern Europe, North Africa and Central Asia |
| Transmission route: Phlebotomine sand flies (Lutzomyia spp. in the Americas and Phlebotomus spp. elsewhere), blood transfusion, venereal and transplacental. |
| Zoonotic: Yes |
Distribution
Leishmania infantum is endemic to the Mediterranean basin, Central Asia, western China, and South America. Canine infections with other species of Leishmania may occur in different countries worldwide [1], including as L. tropica, L. major, L. mexicana, and L. braziliensis, which may cause mainly cutaneous manifestations in dogs.
Clinical signs
Leishmaniosis is a parasitic infection with a wide range of clinical signs. The disease may affect both visceral organs and the skin, or can manifest without skin abnormalities. Dogs and cats may present with visceral and cutaneous manifestations.
The infection outcome depends on the animal’s immune system. Some dogs will eliminate the infection, some will develop subclinical infection and others will develop severe chronic disease. Dogs can present clinical signs or be infected subclinically. Clinical signs may include enlarged lymph nodes, splenomegaly, exfoliative dermatitis, nodular sores on the skin, ulcers, alopecia, conjunctivitis, blindness, epistaxis, muscular atrophy (Fig 1a and 1b).

Figures 1a and 1b Dogs with clinical signs of leishmaniosis (a and b). (Image credit: Prof Dr. G. Baneth)

Skin lesions include multiple ulcerative mucocutaneous lesions, ulcers on the nose, lips, testis and alopecia around eyes.
Diagnosis
Clinical diagnosis may be difficult because clinical signs are variable. Detection of amastigote forms within the cytoplasm of polymorphic nuclear cells or extracellularly in stained smears of skin lesions, bone marrow, spleen or lymph node aspirates, or other infected tissues (Fig 2).
Cytology Detection of amastigote forms within the cytoplasm of polymorphic nuclear cells or extracellularly in
stained smears of skin lesions, bone marrow, spleen or lymph node aspirates, or other infected tissues (Fig 3).
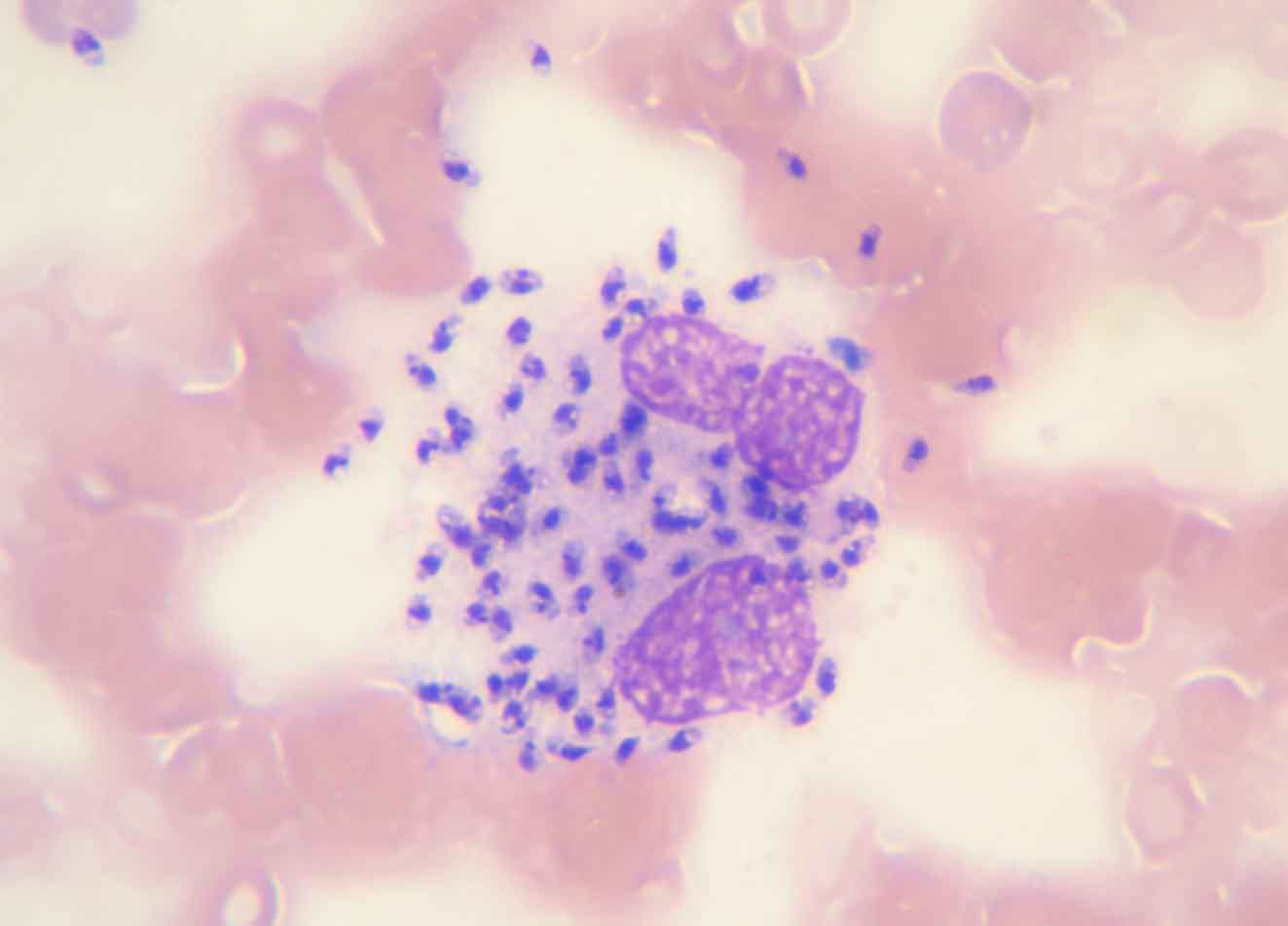
Figure 2 Intracellular and extracellular amastigotes of Leishmania infantum in a splenic smear. (Image credit: Dr.G. Baneth)
Serology is the most common method for diagnosis of dogs with suspected clinical signs of leishmaniosis. oThe immunofluorescent antibody test (IFAT), ELISA, and immunochromatographic assays are the most frequently used tests by veterinarians, although they vary in sensitivity and specificity. It is very important to consider cross-reactivity with other parasitic infections, especially with other Leishmania spp. and Trypanosoma spp. in regions where these parasites are prevalent in dogs (e.g., South America).
The polymerase chain reaction (PCR) is a very sensitive technique for the diagnosis of Leishmania infection but dogs may frequently be positive in dogs from areas where infection is endemic due to subclinical infection. Positive serology has a higher correlation with the presence of clinical disease. For further information, refer to the LeishVet guidelines (http://www.leishvet.org/).
Treatment
Most utilised drug protocols are:
- Meglumine antimoniate (Glucantime) – 75-100 mg/kg, SC, SID for 30 days in combination with allopurinol – 10 mg/kg, PO, BID until clinical signs are not present, haematology and serum biochemistry normalize, and serology reverts to negative.
- Miltefosine (Milteforan) – 2 mg/kg, PO, SID for 30 days in combination with allopurinol – 10mg/kg, PO, BID until all three conditions mentioned above are met.
- Allopurinol alone at 10 mg/kg PO BID in dogs with severe kidney disease or when other drugs are not available.
Control
The main and most effective way to prevent Leishmania infection is through the utilization of topical insecticides including collars and spot-on formulations of pyrethroids.
In countries where efficacious vaccines are marketed, vaccines can be used and started at a young age before exposure to infection. Vaccinated dogs should be negative to infection prior to vaccination and always be protected with topical insecticides.
Prophylaxis can be achieved using all protective methods available. In addition, dogs can be housed indoors from dusk to dawn, ideally in fine mesh netted environments to decrease sand fly bites.
Public health considerations
Several species of Leishmania have been described, most of which are zoonotic. Canines are known as the major host for L. infantum, in both urban and rural environments. Culling of seropositive animals practiced in some countries is controversial due to ethical issues and lack of proven effectivenesseffectiveness.
Public health considerations
[1] Cantacessi C, Dantas-Torres F, Nolan MJ, Otranto D. The past, present, and future of Leishmania genomics and transcriptomics. Trends Parasitol. 2015;31:100-108.